Reviewed By:
Shritej Mali
Independent Research Reviewer
Reviewing peer-reviewed studies and medical literature for evidence-based accuracy.
Written By: Kibo Clinics Content Team
Sources Referenced: American Academy of Dermatology, ISHRS, DermNet NZ, NCBI Bookshelf StatPearls, Cleveland Clinic
Last Updated: June 17, 2026, 2:43 PM IST
Reading Time: 12 minutes
֎ Show Quick Answer AI Quick answer summary
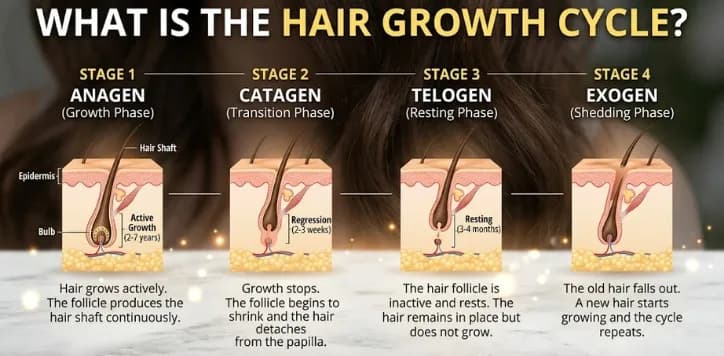
- The hair growth cycle has four practical stages: anagen for growth, catagen for transition, telogen for rest, and exogen for shedding.
- Normal shedding is not always hair loss: many people shed about 50 to 100 hairs daily because follicles do not all cycle together.
- Sudden heavy shedding is usually delayed: stress, fever, illness, childbirth, surgery, crash dieting, or medication changes can push more follicles into telogen, with shedding often showing up weeks to months later.
- Pattern thinning is different from shedding: male pattern baldness and female pattern hair loss usually involve gradual follicle miniaturisation, not just a temporary shedding phase.
- You cannot force the cycle overnight: the right plan is to identify the trigger, correct deficiencies or scalp disease, and treat pattern hair loss early if it is present.
What Is the Hair Growth Cycle?
The hair growth cycle is the repeating biological process that controls how each follicle grows a strand, slows down, rests, sheds the old strand, and starts again. A follicle is not a permanent hair-producing machine. It moves through active and resting states, and the visible hair on your scalp is only the part of that cycle you can see.
The useful point is this: hair fall is not always a sign that the follicle is dead. A strand can shed because it has completed its cycle. It can also shed because illness, stress, hormones, deficiency, medication, scalp inflammation, or pattern hair loss has disturbed the cycle. That is why two people can both say “my hair is falling,” but need completely different next steps.
In normal scalp hair, follicles do not cycle together. Some are growing, some are resting, and some are shedding at the same time. This is why daily shedding can happen without visible loss of density. The concern begins when the amount, pattern, duration, or scalp symptoms change from your usual baseline.
This also explains why treatments take months. A follicle that is resting cannot produce a long visible strand in a few days. It has to re-enter anagen, form a new fibre, and push that fibre through the scalp. If your goal is to understand timelines, this cycle is the base of every honest hair recovery plan.
Evidence basis: ISHRS, “Hair Loss and the Hair Growth Cycle”; DermNet NZ, “Hair Shedding”; NCBI Bookshelf StatPearls, “Physiology, Hair.”
Hair Growth Cycle Stages: Anagen, Catagen, Telogen and Exogen
Most patient-friendly explanations use four stages: anagen, catagen, telogen, and exogen. Some medical texts describe three main phases and treat exogen as the shedding part of telogen. For a reader trying to understand daily shedding, the four-stage version is clearer because it separates “resting” from “falling out.”
| Stage | Simple Meaning | What Happens | Typical Timing |
|---|---|---|---|
| Anagen | Growth phase | The follicle actively produces the hair fibre. This phase builds length and much of visible density. | Usually several years for scalp hair |
| Catagen | Transition phase | Growth slows, the lower follicle regresses, and the strand prepares to move toward rest. | Around 2 to 3 weeks |
| Telogen | Resting phase | The old hair is no longer actively growing, but it may remain anchored while the follicle resets. | Often about 2 to 4 months |
| Exogen | Shedding phase | The old strand releases. You see it on the pillow, comb, shower drain, floor, or clothing. | Part of normal renewal |
Anagen phase: where hair length and density are built
Anagen is the active growth stage. Cells in the lower follicle divide and form the hair shaft. This is the phase that lets scalp hair grow long. A longer anagen phase means a strand can keep growing for more time before it naturally transitions. A shorter anagen phase means the strand may shed before it reaches the length you want.
Most scalp follicles are usually in anagen at any given time. That is why a healthy scalp can keep a stable appearance even while some hairs are shedding. The length of anagen varies with genetics, age, hormones, body site, nutrition, and health. Eyebrow hair stays short because its anagen phase is much shorter than scalp hair.
In male pattern baldness and androgenetic alopecia, sensitive follicles gradually miniaturise. Over repeated cycles, the anagen phase may shorten and the hair shaft becomes finer, shorter, and less visible. This is why pattern thinning is not just “hair fall.” It is a change in follicle behaviour over time.
Catagen phase: the short transition before rest
Catagen is brief. Hair production slows, the lower part of the follicle regresses, and the strand loses the same active support it had in anagen. You usually cannot feel catagen happening. There is no specific “catagen symptom” that a person can spot in the mirror.
The main value of understanding catagen is that it prevents panic. A hair does not suddenly fall the moment growth stops. It transitions, rests, and then sheds later. That delay is why the cause of shedding is often not something that happened yesterday.
Telogen phase: the resting stage that explains delayed shedding
Telogen is the resting phase. The strand is no longer growing, but it can remain in the follicle for weeks or months. When many follicles enter telogen together, the shedding may appear suddenly later. This is the reason a fever, illness, childbirth, crash diet, or emotional stress can be followed by hair fall after a delay.
This delayed pattern is commonly discussed as telogen effluvium. The follicle is usually still alive in this situation. The issue is that too many follicles shifted into rest at the same time. If the trigger stops and no other condition is active, the cycle can gradually rebalance.
Exogen phase: the hair you actually see falling
Exogen is the visible shedding stage. This is the full-length strand you see after washing, brushing, oiling, sleeping, or running your fingers through your hair. A shed strand may have a small pale club-shaped end. That does not mean the living root has been permanently pulled out. The active follicle sits deeper in the scalp.
A wash day can look dramatic because loose telogen hairs collect and come out together. Long hair also looks more alarming than short hair because each shed strand has more visible volume. The important question is not whether any hair came out. The question is whether shedding is far above your baseline, lasting too long, or paired with visible thinning or scalp symptoms.
Evidence basis: ISHRS, “Hair Loss and the Hair Growth Cycle”; DermNet NZ, “Hair Shedding”; Healthline medically reviewed hair-growth-cycle explainer; NCBI Bookshelf StatPearls, “Physiology, Hair.”
How Fast Does Hair Grow?
Scalp hair commonly grows around 1 cm per month, but the visible result depends on more than growth speed. The length you see depends on how long the follicle stays in anagen, how much breakage occurs, how thick each strand is, and whether the follicle is healthy enough to keep producing a strong fibre.
This is why “my hair is not growing” can mean different things. In some people, the hair is growing but breaking before it gains length. In others, anagen may be shortened by age, deficiency, hormonal triggers, or pattern hair loss. In others, frequent shedding makes the ends look thinner even though short regrowth is present near the scalp.
A practical timeline is easier than daily checking. If shedding is triggered by telogen effluvium, it may take months for shedding to settle and months more for new short hairs to create visible density. If pattern hair loss is active, the timeline depends on early diagnosis and whether miniaturised follicles are still responsive. For better tracking, use consistent lighting and monthly photos, not daily mirror checks. This is similar to the process explained in tracking hair growth progress with monthly photos.
| Timeframe | What You May Notice | What It Usually Means |
|---|---|---|
| First few weeks | Shedding may continue even after you correct a trigger. | Old resting hairs may still be releasing. |
| 2 to 3 months | Shedding may begin to reduce if the trigger is gone. | Cycle balance may be improving, but visible density can lag. |
| 3 to 6 months | Short regrowth may become visible around the hairline or parting. | New anagen hairs may be emerging, but they are still short. |
| 6 to 12 months | Density changes become easier to judge. | Hair has had enough time to grow long enough to affect coverage. |
Evidence basis: NCBI Bookshelf StatPearls, “Physiology, Hair”; AAD, “Do you have hair loss or hair shedding?”; Cleveland Clinic, “Telogen Effluvium.”
Normal Shedding vs Hair Loss: The Difference That Matters
Normal shedding means old hairs are leaving the follicle as part of renewal. Hair loss means something is stopping growth, miniaturising the follicle, damaging the hair shaft, inflaming the scalp, or creating bald patches. The two can overlap, but they are not the same.
A person can shed 50 to 100 hairs daily and still maintain density. A person can also shed less than that but still have progressive thinning if the hairs are becoming finer and shorter over time. This is why counting every strand is not always useful. Pattern, density, scalp symptoms, and time course matter more.
| What You Notice | More Likely Normal Shedding | More Likely Hair Loss |
|---|---|---|
| Daily hair fall | Small steady shedding close to your baseline. | Sudden handfuls, persistent heavy shedding, or rapid volume drop. |
| Scalp visibility | Density looks similar overall. | Parting widens, crown shows, temples recede, or bald patches appear. |
| Pattern | Diffuse strands after wash or brushing. | Hairline recession, crown thinning, centre-part widening, patchy loss, or broken short hairs. |
| Scalp symptoms | No pain, redness, scaling, burning, or itching. | Itching, thick flakes, pain, redness, sores, burning, or tenderness. |
For women, hair loss may show as reduced ponytail thickness, widening parting, or scalp visibility rather than a receding hairline. This is covered more deeply in hair loss in women. For men, early recession and crown thinning often need assessment against the Norwood scale and family pattern.
Evidence basis: AAD, “Hair loss: Overview”; AAD, “Do you have hair loss or hair shedding?”; DermNet NZ, “Hair Shedding.”
What Disrupts the Hair Growth Cycle?
The hair cycle reacts to the body’s overall state. Hair is visible and emotionally important, but biologically it is not essential for survival. When the body is under stress, it can temporarily shift follicles away from active growth. That is why fever, surgery, crash dieting, childbirth, emotional stress, illness, medication changes, nutritional deficiency, and thyroid imbalance can show up later as shedding.
The delay is important. According to StatPearls on telogen effluvium, the event that triggers shedding may occur around three months before hair fall begins, but the timeframe can range from one to six months. That means the trigger may already be over by the time hair fall becomes obvious.
| Trigger Type | Examples | How It May Affect the Cycle |
|---|---|---|
| Physical stress | High fever, infection, surgery, major illness, rapid weight loss | Can push more anagen hairs into telogen, causing delayed diffuse shedding. |
| Hormonal change | Postpartum shift, PCOS, menopause, thyroid imbalance | Can shorten growth rhythm, increase shedding, or overlap with pattern thinning. |
| Nutritional gaps | Low iron stores, low vitamin D or B12 risk, low protein intake, restrictive diets | Can reduce follicle support and contribute to diffuse shedding when clinically relevant. |
| Scalp inflammation | Seborrhoeic dermatitis, psoriasis, fungal infection, chronic itching or scaling | Can worsen shedding, breakage, and scalp discomfort; some causes need medical treatment. |
| Genetic sensitivity | Androgenetic alopecia, family history, early hairline or crown thinning | Can gradually shorten anagen and miniaturise follicles over repeated cycles. |
If shedding is diffuse, testing may be useful when symptoms or history point toward deficiency, thyroid disease, metabolic issues, or hormonal imbalance. Kibo’s guide to blood tests for hair fall explains which tests are usually considered for men and women. You can also read more about iron deficiency and ferritin, vitamin D and hair follicles, and biotin supplements for hair growth.
If the scalp has flakes, redness, itching, or soreness, do not treat it as only a vitamin issue. Read whether dandruff causes hair loss, seborrhoeic dermatitis and scalp flaking, and scalp psoriasis versus dandruff for the scalp-inflammation angle.
Evidence basis: NCBI Bookshelf StatPearls, “Telogen Effluvium”; AAD, “Do you have hair loss or hair shedding?”; DermNet NZ, “Hair Shedding.”
Hair Growth Cycle and Common Hair Loss Patterns
The hair cycle helps explain why different types of hair loss behave differently. Some conditions mainly increase shedding. Some shrink follicles slowly. Some damage the shaft. Some cause patches. Treating all of them with the same oil, shampoo, serum, or supplement misses the point.
Telogen effluvium: too many hairs enter rest together
Telogen effluvium is usually diffuse shedding. The hair may come out more during washing, combing, or finger-running, but the scalp often looks otherwise normal. It may happen after fever, surgery, illness, childbirth, crash dieting, major emotional stress, or medication change. Recovery depends on whether the trigger is gone and whether an underlying issue remains active. For a deeper recovery timeline, read hair recovery after telogen effluvium.
Androgenetic alopecia: the cycle slowly shortens
Androgenetic alopecia is different. It is not just temporary shedding. Genetically sensitive follicles gradually miniaturise under androgen influence. The strand becomes finer, shorter, and less pigmented with repeated cycles. Men may notice hairline recession or crown thinning. Women may notice centre-part widening and reduced density. Kibo’s guide to DHT hormone and hair loss explains the hormone side, while DHT blockers for hair loss explains treatment categories.
Alopecia areata: patches are not explained by routine shedding alone
Round or patchy bald spots need a different lens. They can suggest alopecia areata or another localised scalp problem. A normal hair cycle explanation is not enough. These cases need a scalp exam and often trichoscopy. Read alopecia areata explained if the loss is patchy rather than diffuse.
Breakage: hair looks thin even when follicles are cycling
Not all “hair fall” is hair shedding from the root. Heat, friction, chemical damage, tight hairstyles, harsh brushing, and dryness can break the shaft. Broken pieces are often shorter and may not have a club-shaped end. This can make the hair look less dense even when the follicle is still producing hair. If this sounds familiar, compare hair dryer heat and follicle safety, humidity hair texture and breakage, and hair density versus strength.
Postpartum, PCOS and menopause: the cycle can overlap with hormones
Hormonal shifts can move follicles into shedding phases or reveal underlying pattern thinning. Postpartum shedding is often temporary, but it can feel intense. PCOS-related thinning may overlap with androgen sensitivity. Menopause can reduce density and change the growth environment. Useful follow-up guides include postpartum hair loss recovery, PCOS hair thinning in women, and menopause and hair density.
Evidence basis: AAD, “Hair loss: Overview”; AAD, “Do you have hair loss or hair shedding?”; DermNet NZ, “Hair Shedding”; NCBI Bookshelf StatPearls, “Physiology, Hair.”
Want to know whether your hair fall is shedding, breakage, or pattern thinning?
Can You Speed Up or Restart the Hair Growth Cycle?
You cannot safely force hair to grow overnight. The cycle has biological timing. What you can do is remove the factor that is disturbing the cycle, protect the hair shaft from breakage, treat scalp inflammation, correct proven deficiencies, and start medical treatment early if pattern hair loss is active.
Supplements are useful when there is a real deficiency or clinical need. They are not a shortcut for every type of hair loss. Random high-dose supplementation can waste time and may also confuse diagnosis. Oils may improve dryness, smoothness, or scalp comfort for some people, but they do not restart every follicle. That is why guides on rosemary oil for hair growth, castor oil for hair growth, onion juice for hair growth, and rice water for hair growth should be read with realistic expectations.
Medical treatments work best when they match the diagnosis. Minoxidil may support follicles in certain types of hair loss, but it is not the same as correcting iron deficiency or treating scalp psoriasis. Anti-androgen approaches may be relevant in pattern hair loss, but not for every person with sudden shedding. For comparison, read minoxidil versus Redensyl and 5 percent versus 10 percent minoxidil.
At Kibo Clinics, non-surgical options may be discussed when follicles are still active and the diagnosis supports it. These can include PRP therapy, GFC therapy, low-level laser therapy, mesotherapy for hair regrowth, or microneedling for hair regrowth, depending on suitability. If the area is already bald and follicles are no longer producing hair, a medical plan may shift toward surgical evaluation rather than expecting the cycle to restart on its own.
Evidence basis: AAD hair loss diagnosis and treatment guidance; NCBI Bookshelf StatPearls, “Physiology, Hair”; NCBI Bookshelf StatPearls, “Telogen Effluvium.”
Hair Growth Cycle After Hair Transplant
After a hair transplant, growth still follows biology. Transplanted follicles do not instantly produce final density. They go through healing, temporary shedding, resting, early regrowth, thickening, and maturation. This is why judging a transplant too early can create unnecessary anxiety.
Temporary shedding after transplant can happen because grafts experience surgical stress. The follicle remains in the scalp, but the old shaft may shed. Early new growth often appears as fine hair first. Density improves as more follicles cycle into anagen and the shafts thicken over time. Most patients need months, not weeks, to see cosmetic change.
If your concern is transplant planning, the technique, donor strength, graft count, hairline design, and post-procedure care matter. Useful follow-up reading includes FUE hair transplant procedure guide, DHI versus FUE comparison, hair transplant healing and recovery, and documenting your hair journey.
For people with advanced pattern loss, transplant can restore coverage in selected areas, but it does not stop native hair from ageing or miniaturising. The surrounding hair may still need diagnosis and maintenance. This is why surgical planning should include the future pattern, not only the current bald spot.
When Should You See a Dermatologist for Hair Cycle Problems?
See a dermatologist or qualified hair restoration doctor when shedding is heavy, persistent, patterned, patchy, painful, or linked with scalp symptoms. Also seek help if your ponytail feels much thinner, your parting is widening, the crown is becoming visible, the hairline is receding, or you are seeing bald spots.
A good consultation does not jump straight to a serum. It starts with pattern recognition. The doctor looks at your scalp, history, shedding timeline, diet, medicines, recent illness, hormonal symptoms, family history, and hair-care practices. Tests are added when they answer a real question. This is the difference between treating a symptom and finding the cause.
- Sudden diffuse shedding: look for triggers in the last one to six months and consider targeted testing if needed.
- Slow crown or hairline thinning: assess for pattern hair loss and miniaturisation.
- Widening part in women: assess hormones, iron stores, thyroid clues, PCOS signs, and female pattern hair loss.
- Patchy bald spots: do not rely on oils or supplements; get scalp examination and trichoscopy.
- Itching, pain, scaling, or redness: treat the scalp condition, not just the shedding.
If you are confused about whom to consult, this guide on dermatologist versus trichologist explains the difference. If your issue seems local to Mumbai’s environment, read hair loss in Mumbai, Mumbai air pollution and hair protection, and hair fall in monsoon.
Ready to find what is interrupting your hair growth cycle?
Frequently Asked Questions
What are the four stages of the hair growth cycle?
The four practical stages are anagen, catagen, telogen, and exogen. Anagen is growth, catagen is transition, telogen is rest, and exogen is shedding. Some medical explanations use three stages and include exogen within telogen, but the four-stage format is easier for understanding visible hair fall.
How long is the anagen phase of hair growth?
For scalp hair, anagen usually lasts several years. Many references describe broad ranges such as 2 to 6 years or 2 to 8 years because genetics, age, hormones, nutrition, and body site affect the length of the growth phase.
Is it normal to lose hair every day?
Yes. Losing about 50 to 100 hairs a day is commonly considered normal because follicles renew continuously. The concern is sudden heavy shedding, visible thinning, bald patches, scalp symptoms, or a clear change from your usual baseline.
Why does hair fall increase after stress or fever?
Stress, fever, illness, surgery, childbirth, crash dieting, or medication changes can push more follicles into the resting phase. The shedding is often delayed, commonly appearing months after the trigger, because telogen hairs shed later.
Can the hair growth cycle recover after hair fall?
It can recover when the follicle is still active and the trigger is temporary or treatable. Recovery depends on the cause. Telogen shedding can improve after trigger correction, but pattern hair loss usually needs ongoing diagnosis-based management.
Does washing hair disturb the growth cycle?
Washing usually does not create new hair fall. It releases loose hairs that were already ready to shed. If washing is followed by itching, redness, pain, or scaling, the issue may be scalp irritation or inflammation rather than the hair cycle alone.
Can oils or supplements make hair grow faster?
They cannot override the biology of the hair cycle. Supplements help when there is a real deficiency or medical need. Oils may improve dryness or hair feel, but they do not reverse every cause of hair loss. Diagnosis matters before treatment.
How do I know if I am shedding or balding?
Shedding is usually diffuse and temporary. Balding or pattern hair loss usually shows as progressive hairline recession, crown thinning, centre-part widening, or miniaturised fine hairs. A scalp exam and trichoscopy can separate shedding from true thinning.
Does the hair growth cycle change with age?
Yes. The growth phase can shorten with age, and hair fibres may become finer. Hormonal changes, genetics, medical conditions, and scalp health also influence how the cycle behaves over time.
When should I worry about hair fall?
Seek medical assessment if shedding is sudden and heavy, lasts for months, appears with bald patches, causes scalp pain or inflammation, or comes with visible thinning at the hairline, crown, or centre part.
Want a doctor-led diagnosis before trying more products?
Explore Kibo Clinic Services
Hair Transplant: FUE Hair Transplant | Sapphire FUE Hair Transplant | Direct Hair Transplant DHT | Bio FUE Hair Transplant | Real Time FUE Hair Transplant | Corrective Hair Transplant | Hairline Correction | Unshaven Hair Transplant | Body Hair Transplant
Non-Surgical: IV Hair Boosters | PDO Threads Hair Regrowth | Exosomes Therapy
Related Articles
Hair Cycle and Shedding: Anagen Phase Explained | Anagen Phase for Thick Hair | Extend Anagen Phase | Telogen Phase Explained | Telogen Phase and Hair Thinning
Diagnosis and Causes: Shampoo Not Stopping Hair Fall | Frequent Washing and Hair Loss | Anti-DHT Shampoo for Hair Loss | Gut Health and Hair Density | Sugar and Hair Thinning
Growth and Treatment Comparisons: How to Thicken Thin Hair Naturally | Superfoods for Hair Density | GFC Therapy vs PRP | PRP vs PRF for Hair Growth | LLLT Hair Helmet Therapy
Hair Transplant Timelines: Hair Transplant Before and After Timeline | Hair Growth After 3 Months | Hair Transplant Results at 6 Months | Hair Transplant Results at 12 Months
Medical Disclaimer : Information from Kibo Hair Clinics is for educational purposes only. It does not replace diagnosis, trichoscopy, blood test interpretation, prescription treatment, procedure advice, or side-effect counselling from a qualified dermatologist or hair restoration doctor.